Anatomy
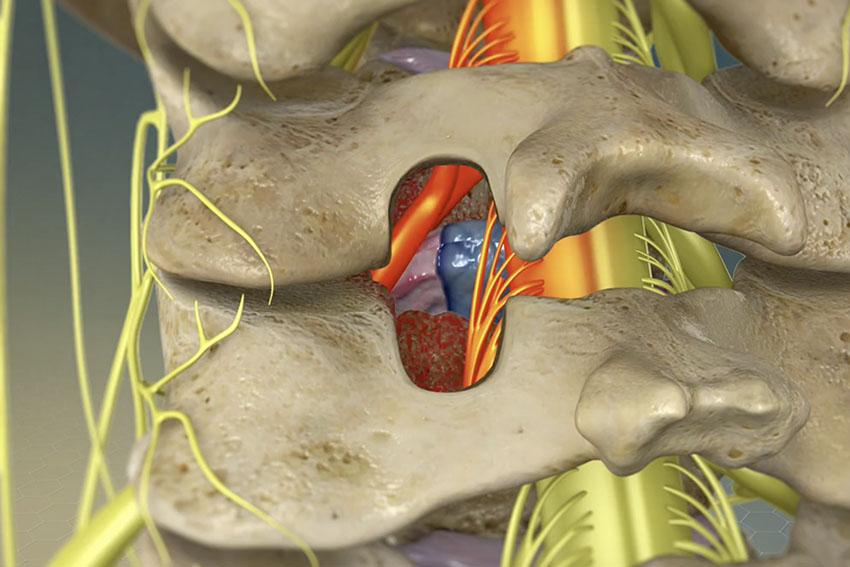
Spinal vertebrae are made up of 3 parts. The front of the vertebrae is made up of the vertebral body and disk. The middle of the vertebrae consists of spinal canal containing the nerves and spinal cord. The back is formed by a protective bone roof called the lamina and spinous process.
The Problem
Disk herniations and bone spurs caused by arthritis can pinch the nerves or spinal cord causing leg pain, numbness and weakness, called sciatica. If they pinch the spinal cord it may myelopathy presenting with pain, weakness and numbness in the arms and legs and difficulty walking even paralysis.
Open Laminotomy
The patient is placed under general anesthetic and positioned face down on the operating room bed. The back is cleaned with antiseptic and sterile draped. X-ray is used to identify the appropriate level of the spinal compression.
The laminotomy can be done with the naked eye or microscope. The main difference is the size of the skin incision and the amount of tissue injury. The microscope and tubular retractors, such as the METRx system from Medtronics, may have an incision 18 to 24 mm in size. Open surgery using the naked eye or microscope may have an incision up to 2 to 4 inches.
A laminotomy is the removal of part of the lamina. The thecal sac and nerves are found by removing the lamina with a drill and the ligament flavum with a Kerrison punch. This allows identifying and removal of the disk herniation or bone spurs relieving pain, suffering, numbness, and weakness. The skin is then closed with sutures and dressing. The patient is usually admitted overnight for observation.
Endoscopic Laminotomy
An endoscopic laminotomy is laminotomy done through 7 to 10 mm incision with the endoscope. This may be done under general anesthesia or twilight sedation. The patient is positioned, prepped and draped as discussed above. Needle is placed onto the lamina of interest under x-ray guidance, which is changed out for K-wire. The skin is incised and series of dilators are used to dilate the skin and place the working port. Under direct visualization the lamina and ligament flavum are removed through the endoscope and the painful disk or bone spur is removed. After complete, the skin is closed with a suture and a bandaid is placed. The patient is usually discharged same day.
Discharge Instructions
- Strict control of sugar diabetes.
- Keep wound clean and dry.
- You may remove your dressing and shower 2 days after surgery. No baths for 2 weeks.
- Watch for the development of fever and redness or drainage from the wound. Call your doctor if you have any concerns.
- Pain, numbness and weakness often require days to months to resolve.
- Return to work, housework and recreational activities as soon as you feel your are able to. Most people can return to work in a few days to few weeks. No lifting greater than 10 to 20 pounds or strenuous activity for the first few months after surgery.