Anatomy
The spine is made up of stacked vertebrae. Each vertebra contains a central open space called the central canal. The central canal contains the spinal cord and spinal in the cervical and thoracic spine and spinal nerves in the lumbar spine.
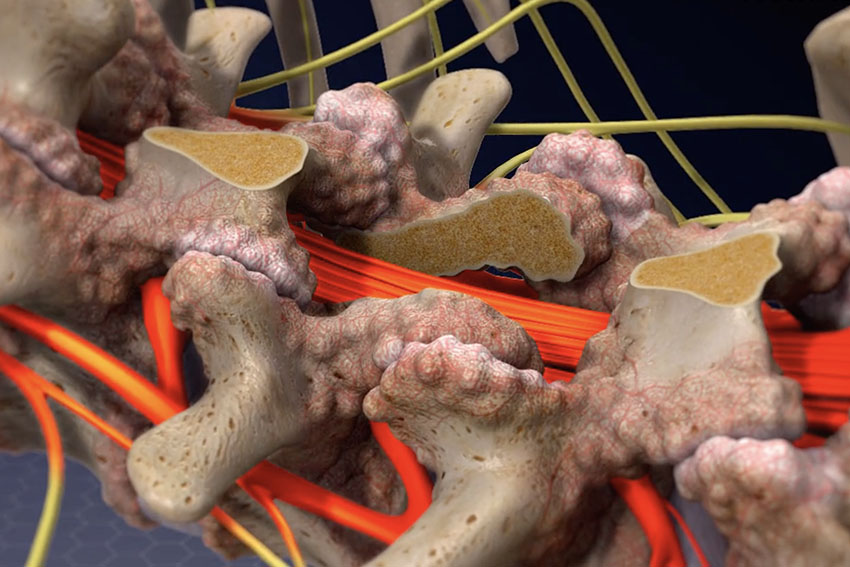
Pathology
Spinal stenosis is the narrowing of the central canal. It usually happens at the level of the disk space in between vertebrae. Spinal stenosis causes pinching or compression of the spinal cord in the upper spine and spinal nerves in the lower spine. Spinal stenosis may present with back pain and leg pain and numbness. If the leg pain and numbness happens mainly with walking this is called neurogenic claudication. This walking pain is relieved with bending forward onto a shopping cart and sitting down. Neurogenic claudication has to be differentiated from vascular claudication, that is similar leg pain caused by narrowed arteries in the legs.
Open Laminectomy
Traditionally spinal stenosis was treated with an open laminectomy. This requires a large 3 to 6 inch midline skin incision, separation and retraction of the back muscles and exposure of the back of the spine. This often leads to significant injury and bleeding in the muscles and soft tissue. The spinous processes, lamina, part of the facet joints and thicken ligament flavum are carefully removed with or without a microscope. The laminectomy is completed after the thecal sac containing the nerves is completely decompressed. The incision has to be closed very carefully to stop and prevent bleeding and restore strength to the incision, usually requiring 3 to 4 layers of sutures. Often a drain has to be left in the incision to prevent blood from accumulating. Post-operatively patients are usually admitted for 2 days to recover from surgery.
Endoscopic Laminectomy
Endoscopic laminectomy is a new procedure done through 1 cm incision with an endoscope. The patient is put under general anesthesia, face down and skin is prepped and draped in sterile fashion. A needle is placed onto the lamina through the back. This is exchanged for a K-wire. 1 cm skin incision is made and the soft tissues are sequentially dilated. This is all done under x-ray visualization. The dilators are replaced with working tube and endoscope. The endoscope allows visualization of the lamina and facet joints and ligament flavum. The lamina at the level of the disk space at the level of the stenosis is carefully removed with electric drill under direct visualization. After this is complete the ligament flavum is removed with biting instruments to decompress the thecal sac and nerve roots. After this is completed the endoscope and tube are removed and the wound is closed with a suture and band aid. Patients may be discharge home or kept overnight for observation.